
Newsletter Apr2026. Upper Cervical Complaints: Dysautonomia & Upper Cervical Instability

Many people struggle with symptoms in the head and neck region. Common symptoms and conditions include chronic neck pain, dizziness, vertigo, tinnitus, migraines and other headaches, TMJ dysfunction, and other orofacial pain. Less common but still frequently seen conditions that can affect the head and neck include Bell’s palsy, Ehlers-Danlos and connective tissue disorders, trigeminal neuralgia, Meniere’s, POTS, and dysautonomia.
Many times, these cases may be related to upper cervical instability. Upper cervical instability is when there is a lack of structural integrity at the base of the skull and the upper neck. This occurs when the joints at the occiput or the first two vertebrae, the atlas (C1) and the axis (C2) are structurally misaligned, have ligamentous laxity or damage, or are functionally unstable.
Symptoms that can be caused by upper cervical instability can include chronic neck pain and stiffness that is not relieved by traditional methods, migraines and cervicogenic headaches, dizziness, fatigue, tingling in the upper extremities, cranial nerve issues, heaviness in the head, vertigo, and others.
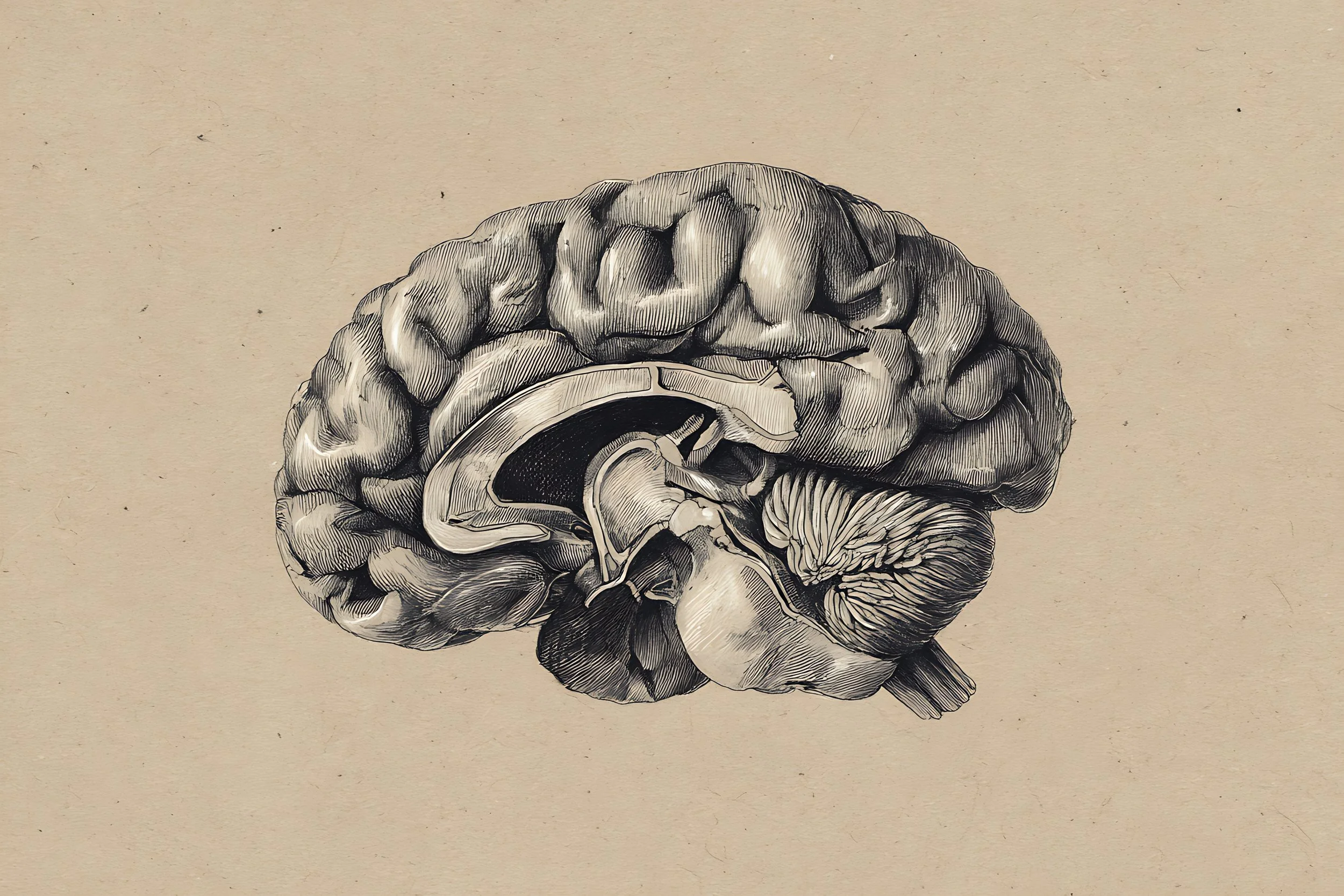
Structural or functional instability in the upper cervical region can occur alongside a host of complex presentations and symptoms that have been historically difficult to treat and diagnose. The atlanto-occipital joint houses the brainstem, which is involved in much of your autonomic nervous system function. The autonomic nervous system is responsible for the ability of your body to maintain a state of homeostasis and manages your breathing, digestion, heart rate, and blood flow. 10 of the 12 cranial nerves that supply the head and neck also originate from the brainstem. The proximity of the brainstem to the upper cervical spine is important because we often see dysautonomia impacted by upper cervical instability.
Homeostasis – maintenance of stable, constant internal conditions through feedback loops that respond to changes by returning variables to a set range (eg, body temperature regulation).
Endocrine systems like the HPA axis (hypothalamic-pituitary-adrenal) are primarily responsible for homeostasis in the body. However, more recently the physiological theory Allostasis has been termed to describe the more complex, adaptative nature of the nervous, immune and endocrine systems’ continual learned response.
Allostasis – The brain’s role in interpreting sensory feedback and making anticipatory adjustments to the body’s physiological processes, effectively preparing for and managing deviations from what might be considered “normal” or baseline conditions. (Joseph P Smith, DC, DACNB).
The endocrine and nervous systems are responsible for communication in the body and are responsible for keeping the body in a state of homeostasis and allostasis. When there is a breakdown in this communication process, the development of dysautonomia and related conditions can occur.
In both the chiropractic and functional medicine models, we seek to support the body’s innate ability to regulate these processes and remove any interference that is hindering the body’s natural abilities.
There can be structural, physiological, chemical, inflammatory/immune, or other factors contributing to symptoms of chronic vertigo, neck pain, fatigue and weakness. Structural changes to the cervical spine can compress the vagus nerve and the vasculature in the neck. Neuroinflammation following TBI (traumatic brain incident) can also be an inciting factor, as well as viral infections, gut-brain axis impairment and metabolic or oxidative stress.
Often, patients have been told that their x-rays and labs are “normal”. Sometimes, this is because of a subclinical presentation without definitive diagnostic markers. Other times, the information has not been assessed in the right way. In either case, we can help promote better function in the body through the holistic, root-cause approach. Upper cervical instability can be structural, or it can be functional, meaning poor proprioception and minute shifts in the upper cervical vertebrae can be causing widespread symptoms even without the presence of ligamentous damage or a disease process.
In our office, we look at health from a functional ability rather than only pathological standpoint.
What does the treatment process for upper cervical instability look like?
Detailed history of symptoms and diagnoses
Subjective evaluations of symptoms and quality of life
Chiropractic evaluation and palpation of the muscles, ligaments and joints of the cervical spine
Possible x-ray analysis to visualize the alignment in your neck while it is in motion
Assessment for localized or systemic hypermobility
Physical exam to assess nutrition, breathing, gait and function
Neurological exam of vestibular, proprioceptive, sensory and motor systems
Advanced laboratory testing if gastrointestinal factors are present
Referral for advanced imaging or specialist consult if indicated
Once we have established what your normal baseline is, we implement a personalized care plan based on your diagnosis. This treatment plan may include:
Specialized, highly specific chiropractic adjustments
Soft tissue manual therapy to release the diaphragm and other soft tissues
Myofascial and craniofacial release
Vagal nerve stimulation
Proprioceptive training and rehabilitation
Lifestyle modifications & referral to other supportive disciplines
Nutritional support based on our findings during your examination
Living with dysfunction in the upper cervical region can be worrying, tiring and painful. However, there are many non-invasive approaches we can take to support your normal function and reduce symptoms that may be impacting your life. The body is incredibly resilient when given the right tools to heal.
References
1. Hope for hypermobility: Part 1—an integrative approach to treating symptomatic joint hypermobility. (n.d.-a). https://www.researchgate.net/publication/369372317_Hope_for_Hypermobility_Part_1-An_Integrative_Approach_to_Treating_Symptomatic_Joint_Hypermobility
2. Hope for hypermobility: Part 2—an integrative approach to treating symptomatic joint hypermobility. (n.d.-b). https://www.researchgate.net/publication/370144194_Hope_for_Hypermobility_Part_2-An_Integrative_Approach_to_Treating_Symptomatic_Joint_Hypermobility
3. EM;, H. J. N. M. (n.d.). Brain mechanisms of HPA axis regulation: Neurocircuitry and feedback in context Richard Kvetnansky lecture. Stress (Amsterdam, Netherlands). https://pubmed.ncbi.nlm.nih.gov/33345670/
4. Hauser, R A, Matias, D., & Rawlings, B. (2024b, November 27). The ligamentous cervical instability etiology of human disease from the forward head-facedown lifestyle: Emphasis on obstruction of fluid flow into and out of the brain. Frontiers in neurology. https://pmc.ncbi.nlm.nih.gov/articles/PMC11638589/
5. Hauser, Ross A, Matias, D., & Rawlings, B. R. (2025, July 2). Cervicovagopathy: Ligamentous cervical instability and dysstructure as a potential etiology for vagus nerve dysfunction in the cause of human symptoms and diseases. Frontiers in neurology. https://pmc.ncbi.nlm.nih.gov/articles/PMC12263383/
6. Healthcare (Basel). (n.d.). Differentiating the structural and functional instability of the craniocervical junction. PubMed. https://na01.safelinks.protection.outlook.com/?url=https%3A%2F%2Fpubmed.ncbi.nlm.nih.gov%2F39408183%2F&data=05%7C02%7C%7Cdc7e3f848e984331769f08de942e5d96%7C84df9e7fe9f640afb435aaaaaaaaaaaa%7C1%7C0%7C639111124023190597%7CUnknown%7CTWFpbGZsb3d8eyJFbXB0eU1hcGkiOnRydWUsIlYiOiIwLjAuMDAwMCIsIlAiOiJXaW4zMiIsIkFOIjoiTWFpbCIsIldUIjoyfQ%3D%3D%7C0%7C%7C%7C&sdata=4LSABTOCOyPuRESCUeDw%2BZ34sFCQ4cpQVIE99Irtl24%3D&reserved=0
7. Kursancew, A. C. S., Faller, C. J., Bortoluzzi, D. P., Niero, L. B., Brandão, B., Danielski, L. G., Petronilho, F., & Generoso, J. S. (2024, December 24). Neuroinflammatory response in the Traumatic Brain Injury: An update - neurochemical research. SpringerLink. https://link.springer.com/article/10.1007/s11064-024-04316-4
8. Libretexts. (2025, June 15). 17.2: An overview of the endocrine system. Medicine LibreTexts. https://med.libretexts.org/Bookshelves/Anatomy_and_Physiology/Anatomy_and_Physiology_2e_(OpenStax)/03%3A_Regulation_Integration_and_Control/17%3A_The_Endocrine_System/17.02%3A_An_Overview_of_the_Endocrine_System
9. Sheng, J. A., Bales, N. J., Myers, S. A., Bautista, A. I., Roueinfar, M., Hale, T. M., & Handa, R. J. (2021, January 13). The hypothalamic-pituitary-adrenal axis: Development, programming actions of hormones, and maternal-fetal interactions. Frontiers in behavioral neuroscience. https://pmc.ncbi.nlm.nih.gov/articles/PMC7838595/
10. Short and long term effects of a two-week transcutaneous vagus nerve stimulation in hyperadrenergic postural orthostatic tachycardia syndrome: A proof-of-concept trial - sciencedirect. (n.d.-c). https://www.sciencedirect.com/science/article/abs/pii/S0953620525004078
11. The communication mechanism of the gut-brain axis and its effect on Central Nervous System Diseases: A systematic review - sciencedirect. (n.d.-d). https://www.sciencedirect.com/science/article/pii/S0753332224010916
12. U.S. National Library of Medicine. (n.d.). National Center for Biotechnology Information. https://pubmed.ncbi.nlm.nih.gov/40387691/
Disclaimer - This document is for informational purposes only and is not intended to provide medical advice, diagnosis, or treatment. Always consult with a qualified healthcare professional before making any changes to your health regimen.