
Newsletter Feb2026. Rethinking Cardiovascular Risk: Evidence for a Metabolic and Functional Medicine Perspective
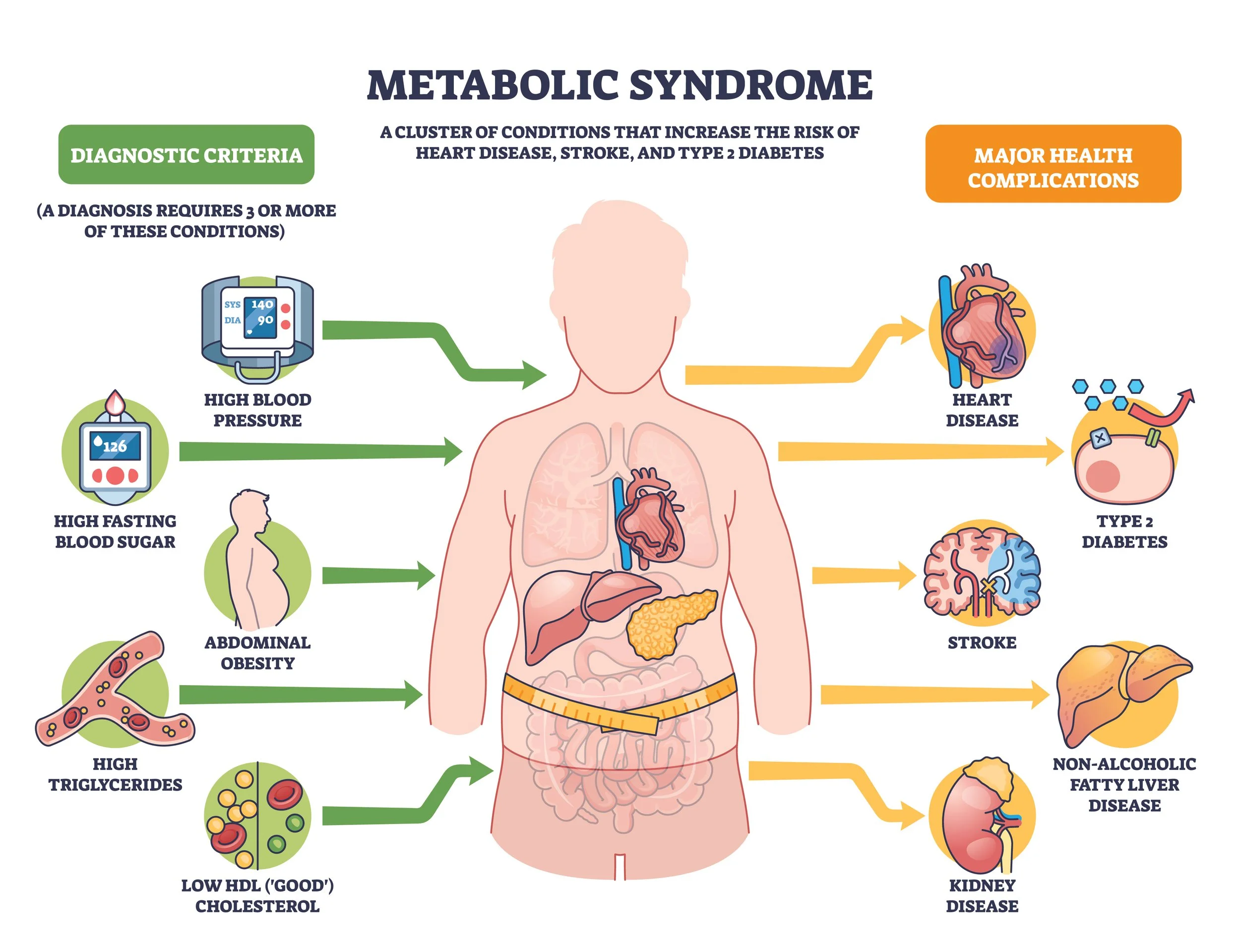
We are so excited to launch ViaVitae Functional Health’s first newsletter this month! February is nationally recognized as American Heart Month, and as whole-body providers we decided to take it one step further to highlight cardiometabolic health since metabolic dysfunction is the root cause cardiovascular disease. We can evaluate metabolic health through regular blood work to identify insulin sensitivity, blood sugar regulation, cholesterol levels, hormones, and inflammation.
Often, cholesterol is the primary focus and while it can be helpful in evaluation of cardiovascular disease (CVD), it should not be considered the all-cause marker for it. In fact, across multiple large population-based cohort studies and systematic reviews, lower low-density lipoprotein cholesterol (LDL-C) levels were not associated with lower all-cause mortality (1,2). Instead, moderate LDL-C concentrations were consistently associated with the lowest mortality, while very low LDL-C levels were frequently associated with higher all-cause mortality, particularly among older adults and in men (2,3,4). In fact, ample cholesterol levels contribute to many healthful processes in our bodies, like hormone production, digestion, and cell membrane formation.
The key is to look at the broad picture in the non-traditional lipid biomarkers, such as lipoprotein (a) [Lp(a)] and apolipoprotein B (ApoB), in combination with the other markers mentioned previously (5,6). Lp(a) shows how genetically prone someone can be to CVD, while ApoB is a protein representing the total number of atherogenic particles, which easily penetrate the arterial wall and oxidize quickly (6,7). These, in combination with C-Reactive Protein (CRP), a marker for inflammation of the blood vessels, and homocysteine, a marker of detoxification, have been shown to be stronger predictors of cardiovascular events than LDL-C alone (8,9,10).
An individual who is going through insulin resistance (high insulin levels) and elevated glucose (blood sugar) levels is at even greater risk of a cardiovascular event (11,12). Insulin resistance leads to an increase in liver production of Very Low Density Lipoprotein (VLDL) levels, which carry and increase triglyceride levels (13,14). This drops HDL production, which reverses cholesterol blood transport used in healthful processes (15,16). Additionally, elevated glucose form metabolic products that damage the blood vessels, increases oxidative stress (imbalance of oxidants to antioxidants), accelerates plaque formation, and activates inflammatory pathways, such as the production of CRP (17,18).
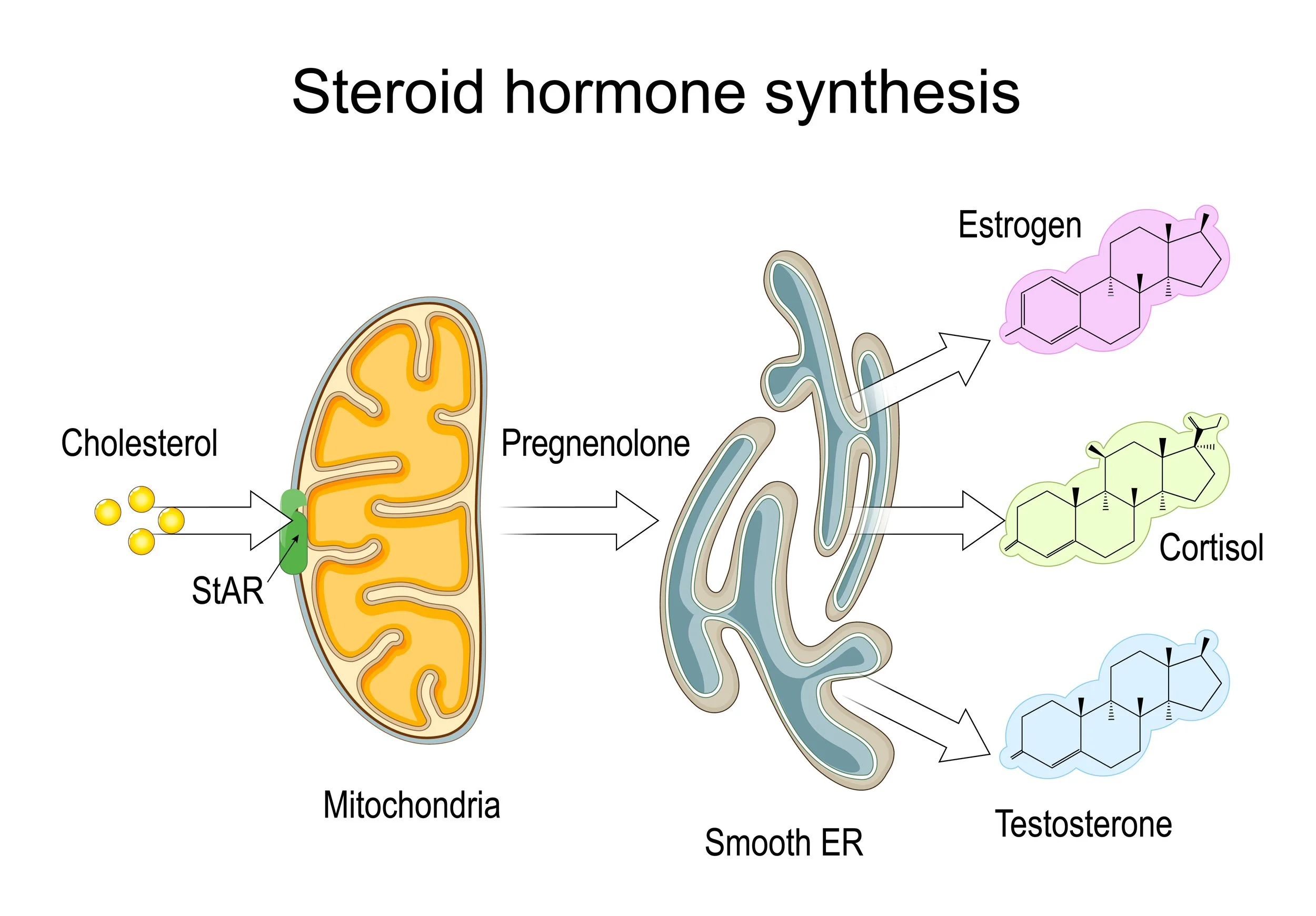
Finally, sex hormones can be an important part of the greater picture of cardiovascular risk (19,20). Adequate cholesterol levels are essential for steroidogenesis, as cholesterol is the foundational precursor for all steroid hormones, including estrogen, progesterone, cortisol, and testosterone. Estrogen has protective effects by supporting blood vessel dilation, reducing LDL oxidation, increasing HDL (“good”) cholesterol, promoting subcutaneous fat over visceral fat, enhancing insulin sensitivity in muscle and liver, and reducing vascular inflammation (19,20,21). This is why women often experience increased cardiovascular risk after menopause (20,21). However, chronically elevated estrogen, especially in synthetic forms from oral contraceptives or hormone replacement therapy, can impair insulin signaling, increase triglycerides (due to liver metabolism of oral forms), promote inflammation (CRP), raise clotting factors, and elevate blood pressure (22,23,24).
Testosterone at optimal levels supports healthy muscle mass and favorable fat distribution, improving the cholesterol profile (25,26). Optimal testosterone also enhances glucose uptake in muscles and reduces insulin resistance (25,27). Low testosterone is associated with insulin resistance, higher triglycerides, lower HDL, increased inflammation, and visceral fat accumulation, all of which contribute to increased cardiovascular risk (26,27,28). Conversely, high-dose testosterone supplementation can be detrimental due to elevated blood pressure and risk of stroke (29).
I could go on, but the key takeaway is that focusing on a single lab value rarely tells the whole story. Taking a systemic, comprehensive view of cardiovascular and metabolic health provides a much clearer picture of true disease risk, which is why we prioritize gathering broad, detailed information from the very beginning at ViaVitae Functional Health.
1. Ravnskov U, Diamond DM, Hama R, Hamazaki T, Hammarskjöld B, Hynes N, Kendrick M, et al. Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review. BMJ Open. 2016;6(6):e010401. https://bmjopen.bmj.com/content/6/6/e010401
2. Bathum L, Depont Christensen R, Engers Pedersen L, Lyngsie Pedersen P, Larsen J, Nexøe J. Association of lipoprotein levels with mortality in subjects aged 50 + without previous diabetes or cardiovascular disease: a population-based register study. Scand J Prim Health Care. 2013;31(3):172–180. doi:10.3109/02813432.2013.824157. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3750440/
3. Kawamoto R, Kikuchi A, Akase T, Ninomiya D, Kumagi T. Low density lipoprotein cholesterol and all-cause mortality rate: findings from a study on Japanese community-dwelling persons. Lipids in Health and Disease. 2021;20:105. https://doi.org/10.1186/s12944-021-01533-6
4. Low-density lipoprotein cholesterol and all-cause mortality: findings from the China Health and Retirement Longitudinal Study (CHARLS). BMJ Open. 2020;10:e036976. https://bmjopen.bmj.com/content/10/8/e036976
5. Tsimikas S, Fazio S, Ferdinand KC, et al. Lipoprotein(a) as a cardiovascular risk factor: current status and future directions. J Am Coll Cardiol. 2018;71(14):1770–1786. https://pubmed.ncbi.nlm.nih.gov/29522809/
6. Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B versus LDL cholesterol in cardiovascular risk prediction. J Clin Lipidol. 2016;10(5):1090–1097. https://pubmed.ncbi.nlm.nih.gov/27840858/
7. Mora S, Cook N, Buring JE, Ridker PM, Lee IM. Combined biomarker score and cardiovascular risk prediction in women. Circulation. 2009;119:1093–1101. https://pubmed.ncbi.nlm.nih.gov/19289614/
8. Ridker PM, Danielson E, Fonseca FAH, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359:2195–2207. https://pubmed.ncbi.nlm.nih.gov/18997196/
9. Zeng Q, Sun F, Zhang X, et al. Lipoprotein(a), C-reactive protein, and traditional lipids: additive prediction of cardiovascular events in a large cohort. Eur Heart J. 2020;41:180–189. https://pubmed.ncbi.nlm.nih.gov/31803033/
10. Emerging Risk Factors Collaboration. Lipoprotein(a) concentration and risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302:412–423. https://pubmed.ncbi.nlm.nih.gov/19602682/
11. Reaven GM. Insulin resistance: the link between obesity and cardiovascular disease. Endocrinol Metab Clin North Am. 2008;37(3):581–601. https://pubmed.ncbi.nlm.nih.gov/18774433/
12. Ginsberg HN. Insulin resistance and cardiovascular disease. J Clin Invest. 2000;106(4):453–458. https://pubmed.ncbi.nlm.nih.gov/10953014/
13. Adiels M, Olofsson SO, Taskinen MR, Boren J. Overproduction of VLDL1 in insulin-resistant subjects is linked to increased plasma triglycerides and small dense LDL. Arterioscler Thromb Vasc Biol. 2006;26(8):1816–1822. https://pubmed.ncbi.nlm.nih.gov/16728569/
14. Taskinen MR. Diabetic dyslipidemia: from basic research to clinical practice. Diabetologia. 2003;46(6):733–749. https://pubmed.ncbi.nlm.nih.gov/12793950/
15. Mooradian AD. Dyslipidemia in type 2 diabetes mellitus. Nat Clin Pract Endocrinol Metab. 2009;5:150–159. https://pubmed.ncbi.nlm.nih.gov/19259185/
16. Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28:629–636. https://pubmed.ncbi.nlm.nih.gov/18239118/
17. Ceriello A. Hyperglycemia and cardiovascular disease: mechanisms and clinical implications. Diabetes Care. 2003;26(5):155–161. https://pubmed.ncbi.nlm.nih.gov/12610090/
18. Howard BV, et al. Insulin resistance, triglycerides, and cardiovascular risk in the Diabetes Heart Study. Circulation. 1996;94:2509–2517. https://pubmed.ncbi.nlm.nih.gov/8898708/
19. Mendelsohn ME, Karas RH. The protective effects of estrogen on the cardiovascular system. N Engl J Med. 2005;353:155–166. https://pubmed.ncbi.nlm.nih.gov/16014812/
20. Vitale C, Mendelsohn ME, Rosano GM. Gender differences in the cardiovascular effect of sex hormones. Nat Rev Cardiol. 2009;6:532–542. https://pubmed.ncbi.nlm.nih.gov/19690538/
21. Miller VM, Black DM, Brinton EA, et al. Menopause and cardiovascular disease risk: the role of estrogen. Endocr Rev. 2007;28:12–36. https://pubmed.ncbi.nlm.nih.gov/17213265/
22. Rosano GM, Vitale C, Marazzi G, Volterrani M. Menopause and cardiovascular disease: the evidence. Climacteric. 2007;10 Suppl 1:19–24. https://pubmed.ncbi.nlm.nih.gov/17439644/
23. Cushman M, et al. Effects of hormone replacement therapy on hemostatic factors in postmenopausal women. Circulation. 1999;100:717–722. https://pubmed.ncbi.nlm.nih.gov/10477518/
24. Canonico M, Plu-Bureau G, Lowe GD, et al. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: meta-analysis. BMJ. 2007;335:1245–1249. https://pubmed.ncbi.nlm.nih.gov/18056655/
25. Caminiti G, Volterrani M, Iellamo F, et al. Effect of long-acting testosterone treatment on functional exercise capacity, skeletal muscle performance, insulin resistance, and baroreflex sensitivity in elderly patients with chronic heart failure. J Am Coll Cardiol. 2009;54:919–927. https://pubmed.ncbi.nlm.nih.gov/19607912/
26. Corona G, Monami M, Rastrelli G, et al. Testosterone and metabolic syndrome: a meta-analysis study. J Sex Med. 2011;8:272–283. https://pubmed.ncbi.nlm.nih.gov/21158846/
27. Traish AM, Saad F, Guay A. The dark side of testosterone deficiency: II. Type 2 diabetes and insulin resistance. J Androl. 2011;32:23–32. https://pubmed.ncbi.nlm.nih.gov/20664187/
28. CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829–1836. https://pubmed.ncbi.nlm.nih.gov/24193080/
29. Vigen R, O’Donnell CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829–1836. https://pubmed.ncbi.nlm.nih.gov/24193080/
Disclaimer - This document is for informational purposes only and is not intended to provide medical advice, diagnosis, or treatment. Always consult with a qualified healthcare professional before making any changes to your health regimen.